Dental Robotics Groupe
WY-5 Series
1.Introduction
2.Treatment Robot
4. History of WY5 Series
In present medical field, there had been a lot of research regarding machine to measure human's mastication movement and machine to measure food's texture. However, these machines only have one particular function and not able to expand their potential to several function.Dental Robotics Group in Takanishi Laboratory, Waseda University had developed mastication robot since 1986 which has the ability to mimic human's mastication movement. Our main purpose in this research is to understand human's mastication movement from engineering point of view.
We also have been developing treatment robot (WY Series) for patients who have mastication movement disorder. This treatment robot use master-slave system and has been a very useful tool for doctors during patient's jaw training compared to the conventional treatment way. In present time, we are developing the fifth robot in this series, WY-5 and this robot has 6 Degree of Freedom (DOF) with parallel mechanism. With this kind of mechanism, the robot has the ability to reproduce the same movable range and force as human's jaw. WY-5 also has the capability to expand its function as Food Texture Measurement Robot WWT-1 (Waseda - Wayo Texturobot-1) beside the function as Treatment Robot for Jaw Disorder Patient WY-5 (Waseda - Yamanashi-5).
2. Treatment Robot
〜WY(Waseda-Yamanashi)5-Series〜
The conventional way of treatment for jaw disorder patient was rely almost on the doctor's experiences and skills. Therefore, we have started our research with objective to develop new system with more effective way and not totally depending on doctor's skills.
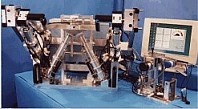
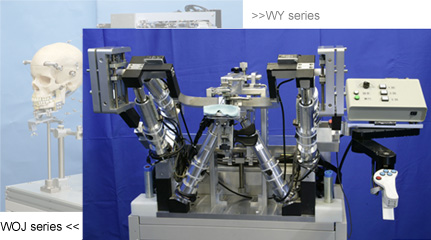
Since 1997, we had developed a 3-DOF treatment robot for jaw disorder person WY-3 (Waseda - Yamanashi-3). This robot was developed based on master-slave system and had the capability for mouth opening and closing training. Furthermore, in order to produce more stable force to the patient jaw during treatment, we had developed WY-5 (Fig. 1) robot with 6-DOF parallel mechanism in 1998.
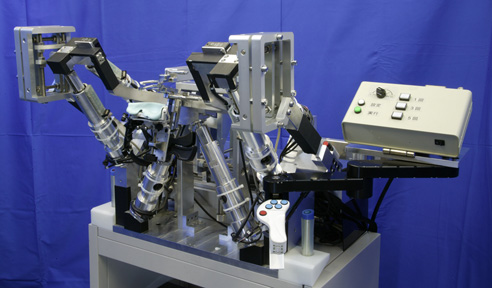
Fig.1 Treatment Robot WY-5RVI
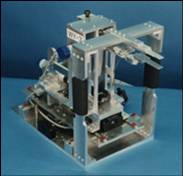
The slave machine's 6-DOF mechanism (Fig. 2) consists of ball screws that are actuated by linear motors. The upper mouth piece will hold patient's upper jaw and patient's lower jaw will be moved accordingly by the movement of parallel link mechanism. This mechanism is more effective than the conventional way using mouth gages that can only perform 1-DOF movement which is opening and closing the mouth. WY-5 treatment robot consists of a slave machine that will move directly the patient's jaw and a master manipulator (Fig. 3) that will be used by the doctor to manipulate the slave machine.
Then, in 2001 we had realized the mouth opening and closing movement, back and forth movement and lateral movement to match the characteristic of human's mouth. In 2002, we had upgraded the treatment capability of this robot by developing new treatment way for openbite disease. Openbite is an insufficient vertical overlap of the teeth. It is caused by oral habits such as tongue thrust, digit sucking, or when the jaws don't grow evenly. Then, in 2003 we had developed EMG feedback monitoring system into WY-5 treatment robot. Using this system, the doctor can monitor EMG feedback in patient’s jaw during the treatment process in this will increase the effectiveness of treatment.In 2004, we upgrade instruments for holding lower jaw which developped in 2002, new one can measure the state of holding lower jaw. We developed a function that can display an improvement in the condition of a symptom in real-time, based upon the data collected during treatment.
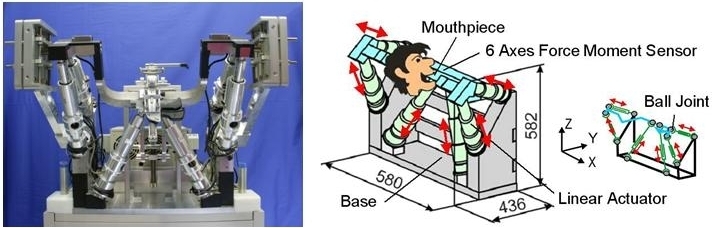
Fig.2 Patient Manipulator
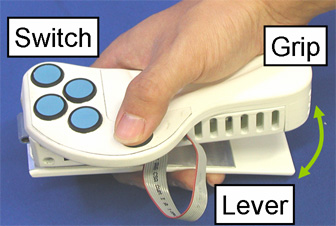 |
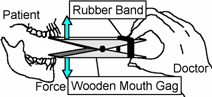 Conventional Treatment with Wooden Mouth Gag 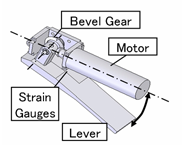 Inside of Doctor Manipulator |
Fig.3 Doctor Manipulator
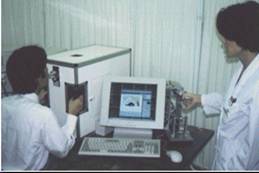
We also had developed tele-training system for WY-5 treatment robot. This system had upgraded the robot capability to do treatment even if the doctor is in distant place. Master manipulator and slave robot are connected through a server and client computer by network using ISDN line. The ISDN line is connected to the robot by dial-up router MN128-SOHO SL11 with speed of 128 Kbps.
Communication between doctor and patient is also important during tele-treatment process. Therefore, we used 3 CCD cameras to transmit patient image to the doctor through videophone and a microphone with a mixer to transmit audio data. By using a mixer, it is possible for more than two persons to communicate using this system. The network composition is shown in Figure 4 and Figure 5.
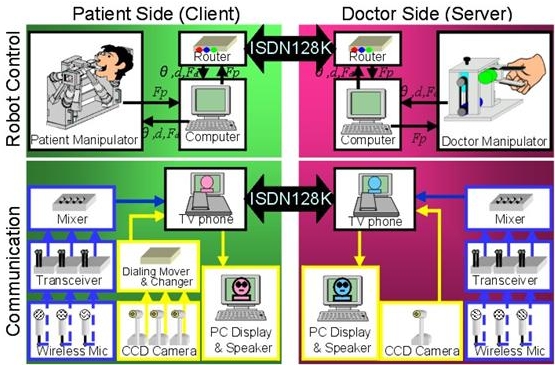
Fig.4 Network Composition of Remote Training
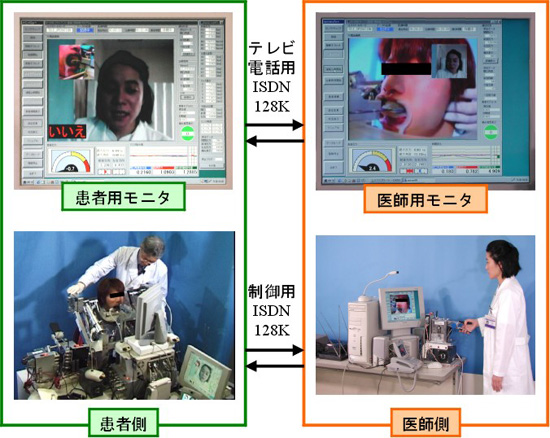
Fig.5 Remote Training with ISDN Line
In order to understand the effectiveness of treatment using WY-5 robot, we had compared the EMG data which is feedback during and after the treatment. We found that the EMG signal after the treatment is lower than during the treatment and we think that the treatment had lower the strain on patient’s jaw muscle. Therefore, we had developed an EMG feedback signal measurement system and this system will increase the effectiveness of treatment by allowing the doctor to monitor any change on patient’s jaw muscle. This system also can help doctor to examine the best way of treatment for particular patient.
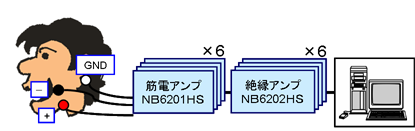
Fig.6 Composition of EMG Signal Feedback System
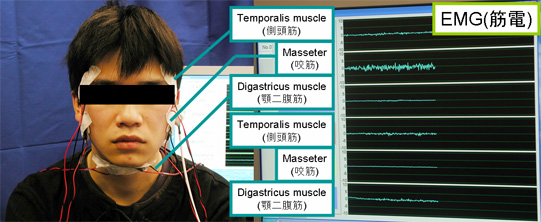
Fig.7 EMG Signal Feedback Interface
++ Instrument for Holding Lower Jaw ++
1. Intermaxillary Traction Therapy
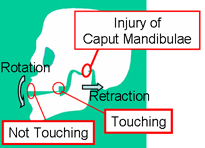
Fig.8 Open Bite
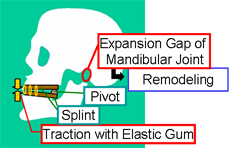
Fig.9 Intermaxillary Traction Therapy
Intermaxillary Traction Therapy is one of the conventional treatment for Open Byte. Openbite is an insufficient vertical overlap of the teeth. It is caused by oral habits such as tongue thrust, digit sucking, or when the jaws don't grow evenly. Fig.9 shows conventional treatment. This treatment method pulls the front tooth with rubber, rotates lower jaw and expands the joint gap. It is thought that the adaptation of the open mouth muscle group and the reproduction of the mandible joint surroundings organization (remodeling) learn by experience to the position of the lower jaw after it pulls it, and this position comes to be maintained. Because of non-physiological movement, if exipasion gap of mandibular joint is only done, the head falls behaind and the mouth opens usually. The treatment is not effective. Therefore we need to hold a patient head to head rest and lower jaw to the patient manipulator. Then we have developed the Instrument for Holding Lower Jaw.
2. Instrument for Holding Lower Jaw
The mold of the mandible of the patient who can prepare the material that is basic in the foundation of the mandible beforehand and make it in a few minutes is fixed and the mandible is fixed by using it the piling.
Moreover, it is necessary to fix the lower jaw firmly to treat effectively. Then, the function to measure the distribution load when the lower jaw was held by arranging the button sensor Nitta Ltd. between the mold and the basement of to measure the holding of the lower jaw was added. The sensor is put in six places. The more power joins, the more the display of the sensor of the display reddens. As a result, the holding get to be understood without depending on patient's sense. (Fig.10, Fig.11)
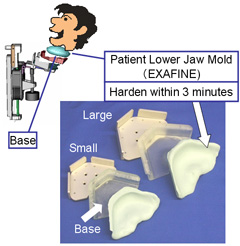 Fig.10 Instrument for Holding Lower Jaw |
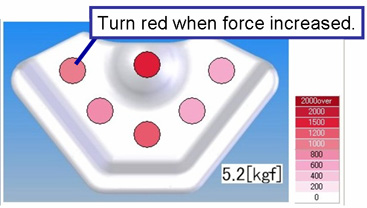 Fig.11 Jaw Holding Force |
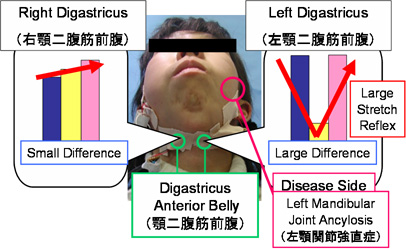
Fig.12 Treatment Evaluation using ARV
The disease that we target is improved by repeating and treating. It is important for patient to continue to have a treatment in aspiringly. The effect was confirmed by the distance of an open mouth that the doctor had measured up to now chiefly before and after treatment with a measuring instrument tool. On the other hand, it was clarified that there was a difference in the treatment data from acquired data depending on the part or the level of the disease when being treating with this robot (Fig.12). Then, we aimed to develop the function of displaying the patient data on the treatment (open mouth reaction force and EMG etc.) and recognizing treatment effect easily.
Fig.13 Change of Traction Distance
On the other hand, the operation of treatment should be constant to display and compare the data such as the open mouth reaction forces and EMG while treating in real time. Then we added the automatic measurement mode. On this mode, robot does specific motion which doctor set. The motion on this mode based on the motion data (Fig.13) which doctor controlled in a previous treatment. The main parameter which doctor set is distance, speed and holding time.
Using this mode, we can measure open mouth reaction force and EMG, display and compare them on time-line. Then, we get to evaluate the treatment effect on real-time (Fig.14).
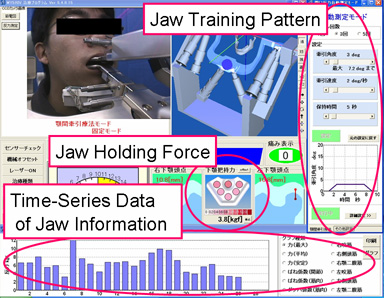
Fig.14 Patient Information Monitoring
3. Food Texture Measurement Robot
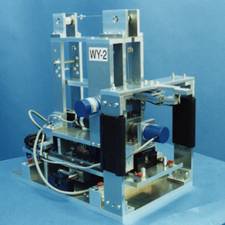
Food had been an important thing in human’s life. Food has 3 main functions which are to support human’s life, stimulate human’s sense and preserve human’s health. Our research on this subject is mainly focus on the second function of food which is related to food texture and human’s sensation. We believe that human’s sensation on food is mainly depends on food texture and so, we had developed two ways to analyze this sensation subjectively and objectively. This research is done by using Universal Dental Robot WY-5 which had been developed in our laboratory. We did some modification and developed new Food Texture Measurement Robot WWT-1 for this research.
There have been a lot of researches regarding this topic, but the food texture measurement machine that had been developed before this robot only had the flexibility of 1-DOF and this limitation make the measurement less effective. Therefore, the merit of WWT-1 which has 6-DOF is the ability to measure food texture by mimicking the human’s mastication movement and this will increase the effectiveness of measurement process.
This robot has a very precise movement with an error range of 0.02 [mm] and by using 6-DOF force sensor that had been integrated in this system, WTW-1 has the ability to detect minimum of 0.001 [N] of force. Therefore, WTW-1 has almost the same performance capability with other measurement machine.
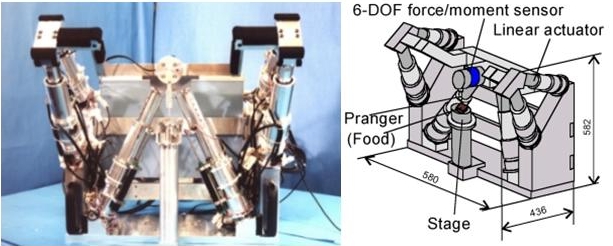
Fig.15 Food Texture Measurement Robot
|
year |
picture |
|
|---|---|---|
|
2001 |
|
|
|
2004 |
|
|
|
2003 |
|
|
|
2002 |
|
|
|
2001 |
|
|
|
2000 |
|
|
|
1999 |
|
|
|
1998 |
|
|
|
1998 |
|
|
|
1997 |
|
|
|
1996 |
|
|
|
1995 |
|
|